A Gender Lens on COVID-19: Investing in Nurses and Other Frontline Health Workers to Improve Health Systems

In a recent CGD blog post, author Megan O’Donnell highlighted seven areas where long-run, gender-responsive thinking can help to insulate against the consequences of pandemics like COVID-19 and their disproportionate impacts on women and girls. Here we take a deeper dive into one of those areas: the promotion of a gender-equal global health workforce in which the occupations where women predominate, such as nursing and community health work, are valued, prioritized, and properly resourced.
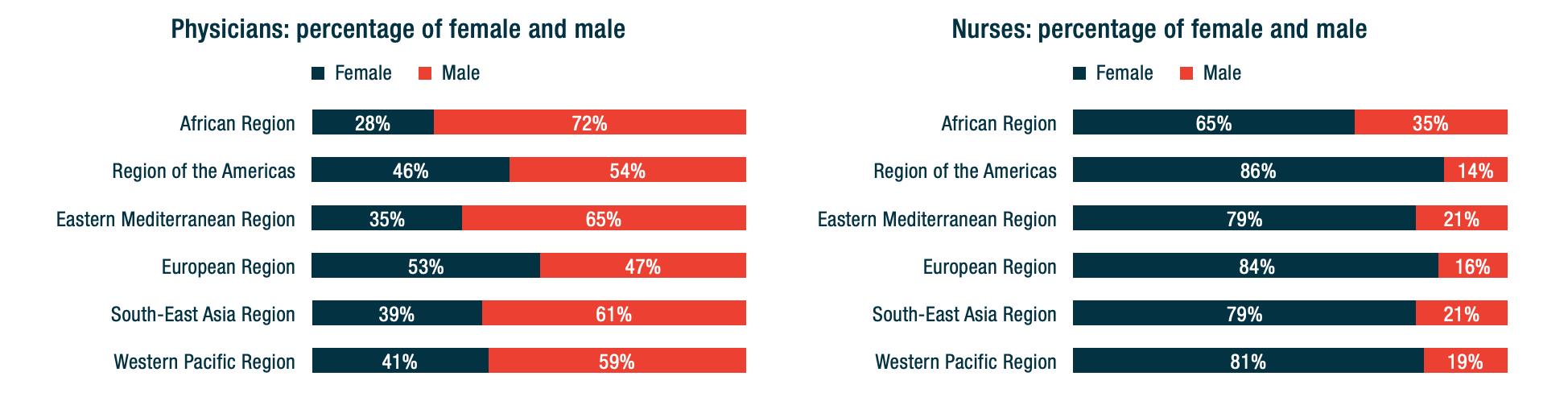
Worldwide, women make up anywhere from 65 percent (Africa) to 86 percent (Americas) of the nursing workforce. Their jobs are critical to the health, safety, and security of communities on any given day, and particularly in times of a global pandemic. And yet, more obviously now than ever before, we face a global nursing shortage. To address this critical short fall and ensure sufficient numbers and distribution of health workers to provide both emergency and routine care in time of crisis, governments need to increase and improve their long-term investment in nurses, including by addressing gender gaps in the health workforce.
- Published in COVID 19, Gender Inequalities, Healthcare
How Will COVID-19 Affect Women and Girls in Low- and Middle-Income Countries?

Policymakers should be thinking—and worried—about how COVID-19 is expected to disproportionately affect women and girls. Gender inequality can come into even starker focus in the context of health emergencies. With COVID-19 continuing to spread, what do we see so far—and what can we expect in the future—in terms of the impacts on women and girls?
Wenham, Smith, and Morgan discuss gendered impacts in their article, “COVID-19: the gendered impacts of the outbreak,” in the Lancet. Women appear to be less likely to die from COVID-19: “Emerging evidence suggests that more men than women are dying, potentially due to sex-based immunological or gendered differences, such as patterns and prevalence of smoking.” But keep in mind that “current sex-disaggregated data are incomplete, cautioning against early assumptions.” In other research, data from 1,000+ patients in China show that “41.9% of the patients were female.” (Guan and others 2020). But beyond these direct effects, most of the other impacts affect women negatively and disproportionately.
Wenham, Smith, and Morgan highlight that women will be more affected in places with more female health workers. In an analysis of 104 countries, Boniol and others (2019) show that women form 67 percent of the health workforce (see the figure below). In China, “an estimated 3000 health care workers have been infected and at least 22 have died” (Adams and Walls 2020). As the pandemic spreads, the toll on women health workers will likely be significant.
Figure. Gender distribution of health workers across 104 countries
Source: Boniol and others (2019)
Here are other areas highlighted by Wenham, Smith, and Morgan:
– School closures are likely to have a differential impact on women, who in many societies take principal responsibility for children. Women’s participation in work outside the home is likely to fall. (My colleagues Minardi, Hares, and Crawfurd have written about other impacts of school closures during an epidemic.)
-Travel restrictions will affect female foreign domestic workers. Of course, they also affect male migrants. The distribution will vary by country. Research by Korkoya and Wreh (2015) found that 70 percent of small-scale traders in Liberia are women, so domestic travel restrictions during the Ebola outbreak disproportionately affected women.
-Health resources normally dedicated to reproductive health go towards emergency response. During the Ebola outbreak in Sierra Leone, for example, the “decrease in utilization of life-saving health services translates to 3600 additional maternal, neonatal and stillbirth deaths in the year 2014-15 under the most conservative scenario” (Sochas, Channon, and Nam 2017). In my own research (with Goldstein and Popova), we found that the disproportionate loss of health workers in areas that had few to begin with would likely lead to higher maternal mortality for years to come.
-When women have less decision-making power than men, either in households or in government, then women’s needs during an epidemic are less likely to be met.
Here are four additional concerns:
-Sexual health: During the school closures of Sierra Leone’s Ebola outbreak, “a reported increase in adolescent pregnancies during the outbreak has been attributed largely to the closure of schools.” (UNDP 2015). Bandiera and others find that in villages highly disrupted by Ebola, girls were “10.7 percentage points more likely to be become pregnant, with most of these pregnancies occurring out of wedlock.” A United Nations report gives an even higher estimate of 65 percent. The absorption of health resources by emergency response may also lead to disruptions in access to reproductive health services.
Many girls didn’t return to schools once they reopened, and there were increases in unwanted sex and transactional sex. (Notably, Bandiera and others also find that girls in villages where there were established “girls’ clubs”—safe spaces for teenage and young adult girls to gather and get job and life skills—before the epidemic experienced fewer of these adverse effects.)
-Intimate partner violence rises in the wake of emergencies: Parkinson and Clare document a 53 percent rise in the wake of an earthquake in New Zealand and nearly a doubling in the wake of Hurricane Katrina in the United States. Mobarak and Ramos find that in Bangladesh, increased seasonal migration reduces intimate partner violence, at least in part because women spend less time with the potential perpetrators of that violence. Travel restrictions may be expected to have the opposite effect.
-The burden of care usually falls on women—not just for children in the face of school closures, but also for extended family members. As family members fall ill, women are more likely to provide care for them (as documented during an Ebola outbreak in Liberia, with AIDS patients in Uganda, and in many other places), putting themselves at higher risk of exposure as well as sacrificing their time. Women are also more likely to be burdened with household tasks, which increase with more people staying at home during a quarantine.
-As Mead Over and I have discussed, health crises can trigger economic crises. Economic crises affect women disproportionately, particularly in low-income countries. Sabarwal and others found that men’s labor force participation remained largely unchanged during economic crises, whereas women’s labor force participation rose in the poorest households and fell in richer households.
-Last week, the World Health Organization declared that “this is the first pandemic caused by a coronavirus.” There have been more than 168,000 confirmed cases and more than 6,600 deaths in 148 countries as of publication of this blog. The impact of this pandemic will be felt for years to come. As women are often disproportionately affected by the follow-on effects of the disease, we have to make sure that we keep women’s rights and needs front and center in our responses. A first step in doing that is making sure that women are a central part of the teams designing those responses.
Contributed by David Evans, senior fellow at the Center for Global Development, working on education, health, and social safety nets.
This post benefitted from comments provided by Susannah Hares, Megan O’Donnell, Emily Christensen Rand, and Rachel Silverman.
Original blog published on Center for Global Development website March 16, 2020, see here for the original posting
Reposted with permission from David Evans, senior fellow at the Center for Global Development
- Published in COVID 19, Healthcare
The Homemade Value-Added Stabilizer

“Shelter in place” mandates in the early stages of the U.S. Covid-19 pandemic required many people to stay home, cook their own meals, school their own children, and entertain themselves. Unpaid work served not only as a social safety net, but also as an automatic stabilizer. While it didn’t dampen fluctuations in official Gross Domestic Product, as did unemployment insurance, it clearly helped stabilize consumption.
Just imagine what would have happened if most people had not had refrigerators, stoves, and computers—or just read reports of the plight of homeless people.
By mid-March 2020, many states and localities shut down restaurants for any services other than take-out. Home-produced meals increased of necessity. Many such meals probably consisted of convenient processed foods that could be popped into a microwave oven, but a renaissance of home cooking also became apparent, along with reliance on long-lasting, easily stored items such as rice and beans. Analysis of Google Search terms showed a sharp spike in questions concerning food preparation and storage. As one newspaper put it, America began baking its heart out. Yeast suddenly became as hard to come by as toilet paper.
In 2018, according to the American Time Use Survey, adult civilian women spent an average of .8 hours a day, and their male counterparts .4 hours a day in meal preparation. How much more did they spend in the months of March and April, and what was the monetary value of this unpaid labor, based on what it would have cost them to hire someone to plan, cook, and clean up? How much did they save on eating-out?
Many childcare centers and schools were closed, leaving parents with responsibility for home-schooling, supervising children, and keeping them from going confinement-crazy. The American Time Use Survey averaged the amount of reported time that married mothers and fathers living with children under the age of 18 spent in primary activities of caring for and helping household children over the 2013-2017 period—an average of 2.6 hours per day for mothers not employed and 1.4 hours for fathers not employed.
Under sequestration, both active care and supervisory care (defined as the time in which an adult reported that a child under the age of 13 “in their care” ) ballooned. How much did these two forms of childcare increase? How much did households save on childcare costs?
Video streaming and gaming increased dramatically, especially during afternoon hours, and people began to rely more heavily on streaming for instruction and exercise as well as entertainment. So, while they spent less money (and less travel time) on entertainment away from home, they substituted forms of entertainment that were probably less expensive, on average. How much less expensive?
Between March and May, average household income plummeted as a result of job furloughs and unemployment. The increase in time devoted to household production buffered this loss to some extent—but without answers to the questions above, we can’t know how much. Most recent impromptu household surveys have focused primarily on women’s unpaid work relative to men’s—an important, but different topic.
For years, I have protested economists’ lack of interest in total consumption—defined as the sum of money expenditures and the consumption of home-produced services.
Let me will repeat one example that I have written about in more detail elsewhere: Compare two couples, each with two small children, each earning $50,000 after taxes. Conventional measures treat them as having exactly the same income. Yet one couple may include an adult earning $50,000 and a full-time homemaker/caregiver, while the other includes two adults earning $25,000 each and obviously has less time to devote to unpaid work. If we assigned any positive value to unpaid work, the first household would obviously be better off in terms of both income and consumption.
Market income is just not a very good indicator of total consumption among households with differing inputs of unpaid work. Also, the value of unpaid work is greater in households with more than one person, because of economies of scale in food preparation and childcare. Standard equivalence scales used to adjust household income for household size and composition completely ignore these issues.
Obviously, the additional unpaid work performed while sheltering in place was a source of great stress, especially for those simultaneously telecommuting, zooming, or otherwise trying to fulfill paid employment responsibilities at home. Yet, it’s hard to deny that this work also “added value,” enabling an important form of social provisioning.
The worst-case scenario for a household with children was almost certainly one in which all adults (e.g. mother and father) were essential workers, required to keep working (often at risk to their health) but unable to work from home. Federal and state agencies tried to provide “resources” for these workers, but no guarantees were forthcoming.
In many cases, one of the adults (probably the mother) was forced to quit or take a leave of absence from paid employment. While new federal legislation gives states flexibility to pay benefits where an individual leaves employment to care for a family member, not all states do so.
Such a policy is effectively a paid family leave—something that most states have shied away from for years, making this country an international outlier. The complexity of the new legislation, plus the difficulty of actually filing for and receiving unemployment benefits, has probably kept take-up pretty low even in states that allow this option.
Just one more reason to consider policies such as federal paid family and sick leaves and a universal basic income that could help the stabilizers known as households do their job.
Original blog published on CARE TALK: FEMINIST AND POLITICAL ECONOMY on May 19th, 2020. See here for the original posting.
Reposted with permission from Dr. Nancy Folbre from University of Massachusetts Amherst and an expert researcher for the Care Work and the Economy Project within the Rethinking Macroeconomics working group.
- Published in COVID 19, Time Use Survey, U.S., Unpaid Work
Playing the Long Game: How a Gender Lens Can Mitigate Harm Caused by Pandemics

When crisis hits, longer-term thinking can easily, and understandably, be cast as a distraction or a luxury—even when it relates to tackling critical issues like gender inequality, climate change, or extreme poverty.
Speaking personally, I’ve felt a bit silly trying to push forward projects that focus on gender lens investing or women’s economic empowerment in the last few weeks, given that my colleagues’ and collaborators’ attention, and frankly much of my own, lies elsewhere, and with something that seems much more pressing.
But for those of us who are in the position of privilege to continue thinking long term, it’s our responsibility to do so. Working towards structural changes that will take longer to come to fruition, especially those that relate to reducing global inequality, is the only way to radically decrease the extent of harm caused by moments of crisis, especially for vulnerable populations.
Dismantling unequal power structures, and in turn ensuring that every individual—regardless of gender, age, income level, national origin, and so on—has a safety net protecting them from vulnerability to health scares, income loss, and threats of increased violence, will allow us to focus on crisis without fearing fallout across every dimension of life.
In times of pandemic, the economically vulnerable cannot afford to stay home. Women in quarantine are facing increased risks of intimate partner violence. Girls staying home from school in some parts of the world may not have the opportunity to return. And none of this would be the case if we more effectively tackled the forms of inequality that underlie these realities. Then a virus could be a virus — assuredly deadly and destructive from a health perspective – but without inciting increased abuse, poverty, and lost prospects.
My colleague David Evans, drawing upon work by Claire Wenham, Julia Smith, and Rosemary Morgan in The Lancet, recently highlighted a range of problems stemming from the COVID-19 pandemic that disproportionately impact women and girls. In hopes of continuing to move the conversation forward, I propose some solutions to those problems here, and welcome others to add to this initial list. To be clear, these actions should not distract from immediate measures to address the pandemic. But we also can’t afford to risk forgetting about them when the focus on COVID-19 has faded; otherwise history is doomed to repeat itself.
1. Promote a Gender-Equal Health Workforce
Because the health workforce is disproportionately women (67%), women are at a higher risk of exposure to the virus within medical facilities.
More doctors worldwide are still men. But the vast majority of the global health workforce consists of nurses, community health workers, and others who are less highly compensated. All health workforce jobs need to become increasingly well-compensated, high-quality jobs. Not only will this incentivize men to seek these positions, destigmatizing their current positioning as “feminine” and dismantling occupational sex segregation within the healthcare sector, but it will also ensure that those on the frontlines of protecting populations from pandemics don’t also have to fear economic fallout on a day-to-day basis.
The number of women doctors is rising. Research from other sectors tells us what works to combat occupational sex segregation, including men acting as mentors supporting women to “cross over” into higher-paying occupations. These efforts will have to be paired with those that increase the perceived (and actual) value of work in sectors, including nursing and other frontline health work, where women dominate. More research is needed on this front, both on what works to incentivize men to take up traditionally “feminine” roles and how to avoid unintended displacement of women from those occupations.
2. Protect (and Expand) Existing Health Resources
With all hands on deck to fight COVID-19, particular groups of women and girls face other health risks.
Health facilities should not have to choose between providing lifesaving care in the face of pandemics and continuing to provide support for those in need in other areas, including pregnant women, adolescent girls (who have the highest prevalence of HIV infection, and in need of life-saving medication to keep their immune systems strong), and all women and girls in need of contraceptive access.
Increased investments in health are needed to ensure critical day-to-day care is not compromised during times of crisis. Establishing a Global Health Security Challenge Fund would help ensure countries are prepared to balance day-to-day needs with additional burdens in the face of pandemic, and evidence-based prioritization strategies are needed for when resources cannot be expanded.
3. Reduce and Redistribute Unpaid Care Work Burdens
As schools close and people fall ill, women and girls will assume increased unpaid care work burdens.
Under business-as-usual scenarios, women and girls do more than their fair share of unpaid care work, which limits their educational attainment, workforce participation and advancement, and leisure time. To lessen these burdens in times of crisis and more generally, we need increased investments in child and elder care, and in the poorest countries, gender-responsive energy, water, and sanitation infrastructure that would reduce the time women and girls must spend collecting water and fuel, as well as cooking and cleaning. We also need shifts in household norms that mean men assume more unpaid care responsibilities. Initiatives focused on promoting women’s economic empowerment, such as 2X Challenge and the Women’s Global Development and Prosperity (W-GDP) initiative, as well broader investments in gender equality and economic growth, must prioritize reducing and redistributing women and girls’ unpaid care work.
4. Address Gender-Based Violence
With quarantine measures imposed and stress heightened, women are at increased risk of violence committed by their partners and family members, and essential support services are absent.
Early reports suggest that gender-based violence rates are increasing in light of COVID-19 quarantining, consistent with evidence documenting increased violence in other crisis settings. Gender-based violence needs to be elevated as its own public health crisis, and resourced accordingly.
We’re far from meeting this objective, considering that all OECD donors combined allocated less than $200 million to addressing violence against women according to 2016-17 data, and over half of this financing came from just three countries (Australia, Canada, and Norway). Increased resources should target evidence-based approaches, such as Promundo’s MenCare program.
In pandemic contexts, preparations for social distancing should include considerations of how individuals will be able to access social services when faced with violence in their households. The World Bank has taken a step in the right direction in positioning interpersonal and gender-based violence as priorities to address in its new Fragility, Conflict, and Violence Strategy, though time will tell how the bank and other donor institutions finance this priority.
5. Guarantee Girls’ Education
With schools closing as part of social distancing measures, girls who already face pressure to drop out of school may not return.
Even absent crisis, tens of millions of girls globally face pressures to drop out of school to care for siblings and do other unpaid domestic work, contribute to supporting their households financially, and/or marry and have children when they are still children themselves. These pressures may be heightened due to interruptions in their education, as observed when Ebola hit West Africa. School closures, especially those impacting adolescent girls, should be weighed against longer-term risks related to girls’ school drop-out and limited school-to-work transition prospects as a result. Where possible, efforts should be made to incentivize parents to allow their children to return to school and to ensure consistent access to sexual and reproductive health services in the interim, as unintended pregnancy is cited as a reason for girls’ failure to return to school.
6. Promote Women’s Economic Opportunities
Across the globe, women are more likely to work jobs that are low-paid, informal, and lacking in benefits.
In large part due to the disproportionate unpaid care work women take on, they are less likely to be employed full-time, in the formal workforce, or in jobs that provide paid sick leave, unemployment insurance, and other protections.
We must continue to invest in evidence-based programs and policies that improve women’s economic opportunities and support organizations such as the Self-Employed Women’s Association and Women in Informal Employment: Globalizing and Organizing—organizations that are well-positioned to provide and advocate for dignified work.
Cash transfers should be considered as a means of ensuring a social safety net for those most in need. Critical to transfers’ success will be (1) ensuring that delivery mechanisms (through digital technology or otherwise) are properly designed and implemented and (2) that those in need, including low-income populations and workers vulnerable to economic backslides because of the virus, are prioritized.
7. Ensure Women’s Representation in Decision-Making and Critical Research
Women are not equally represented in decision-making roles responding to the COVID-19 pandemic.
The White House Coronavirus Task Force is over 90 percent men, and the team Prime Minister Johnson just assembled to lead the United Kingdom’s COVID-19 response is all men. As in the contexts of peace and security, international trade, and climate change, an exclusionary approach to decision-making will yield inferior decisions: those that don’t account for the needs and constraints of populations absent from the table.
Going forward, decision-making teams should be equally representative of men and women, and also prioritize other forms of inclusion, such as those based on race and ethnicity, as called for by Women in Global Health’s Operation 50/50 campaign.
Women must also be equally represented in clinical trials as biomedical treatments and other interventions are developed. As my colleague Carleigh Krubiner has noted speaking to the context of Ebola, women who are pregnant or breastfeeding are typically excluded from experimental studies, and in some high-fertility contexts, this means up to 80 percent of reproductive age women are virtually invisible in trial samples. Lack of representation means a lack of essential data on the types of prevention methods, treatments, and other interventions that work for women, risking higher fatality rates and other complications.
Times of crisis magnify the cracks in our systems and highlight disproportionate risks to the most vulnerable among us. COVID-19’s impacts, those already felt as well as those still anticipated, should serve as a wake-up call. They should spur action to address underlying inequalities, including those that disadvantage women and girls worldwide and make the consequences of a pandemic even worse than they would otherwise be. Increased prioritization of women and girls’ health, education, economic opportunity, safety, and decision-making power can help create a world where no one falls through the cracks. Decision-makers should realize this is inextricably linked to today’s pandemic response.
Contributed by Megan O’Donnell Assistant Director, Gender Program and Senior Policy Analyst at Center for Global Development
Original blog published on Center for Global Development website March 18, 2020, see here for the original post
Reposted with permission from Megan O’Donnell Assistant Director, Gender Program and Senior Policy Analyst at Center for Global Development
- Published in COVID 19, Gender-Equal Economy, Healthcare
Invisible Frontliners: Migrant Care Workers in the Time of COVID-19

The Covid-19 pandemic has exposed fault lines in national healthcare and social protection systems that have made many countries – developed as well as developing – unable to quickly and efficiently deal with this new health crisis and its disastrous consequences on jobs and incomes. One segment of the population in Europe, North America and Asia’s wealthy countries is falling deep into these crevasses, and, sadly, is missing from national debates and policy agendas on the Covid-19 crisis. This group comprises the migrant care workers, especially those who provide care services to elderly, frail, and dependent persons in caregiving institutions and private homes.
Overwhelmingly consisting of women, these migrant workers (along with minority ethnic groups) are the backbone of the childcare, elderly care and long-term care sectors. They include “nannies”, “home carers”, “social care workers”, “collaboratrice familiar”, nurses and nursing aides, among others. According to the European Commission, workers engaged in “personal and household services” are mostly women, working mainly part-time and often of migrant background. ILO estimates that globally there are 11.5 million international migrant domestic workers, and nearly 80 percent of them are employed in OECD countries. According to data on OECD countries, in 2012–13 28 percent of home-based caregivers were foreign-born.
Increasingly restrictive immigration controls in high-income countries in the past two decades have channelled a disproportionate share of immigrants into jobs in informal long-term and home-based care where wages are low, work hours are long and unpredictable, protection from abuse may be missing, and workload is heavy.[1] These are jobs that can easily be concealed from government surveillance. In the US, UK and Canada, for example, most foreign-born care workers enter the country through non-employment routes, such as family unification, refugee protection and asylum programs, and are on student, tourist and working holiday visas. An unknown number of them work clandestinely.
These migrant care workers are particularly vulnerable in the current Covid-19 pandemic for several reasons. First, eldercare homes across Europe and North America have emerged as hotspots of COVID-19 cases and account for a disproportionate share of deaths related to COVID-19. Data collated by the International Long-term Care Policy Network (hosted by the London School of Economics) across five European countries suggest that between 42 and 57 percent of deaths related to COVID-19 have so far occurred in nursing homes.
Secondly, the disproportionate and increasing share of COVID-19 deaths in eldercare homes is not simply due to the residents’ higher vulnerability due to their age and health conditions. It is also because many caregivers in these homes lack access to PPEs and are often overworked in often understaffed facilities. Being poorly paid, some of them also work in multiple facilities just to make ends meet. Poor working conditions of migrant workers in long-term and eldercare homes have been well documented by several studies – conditions regarding their work hours, allocation of responsibilities for diverse tasks and more difficult patients, low pay rates, and no overtime compensation.
Thirdly, the hundreds of thousands of migrant domestic workers who work in private homes are in the frontlines of keeping homes safe and clean. They face multiple risks as a result of the pandemic – health risks, more demands on their time, and income loss. According to the International Domestic Workers Federation, domestic workers worldwide have reported many concerns since the global pandemic began. With entire families staying home all day due to quarantine measures, domestic workers face heavier demands of cooking, cleaning, and caregiving without the benefit of additional pay for longer hours—and because of mobility restrictions, many cannot leave the homes where they work.
Finally, many care workers who have irregular migrant and/or employment status under informal arrangements have no access to unemployment and health insurance benefits, relief packages or financial aid related to COVID-19. This has been recently documented by the National Domestic Workers Alliance and the Pennsylvania Domestic Workers Alliance (networks representing nannies, caregivers and domestic workers in the US), the European Trade Union, and the Kanlungan Filipino Consortium in the UK. Those who fall ill prefer not to go to hospitals until it is too late for fear of being reported to migration authorities and because they do not have health insurance. These care frontliners are largely invisible and likely to suffer in silence
Contributed by Amy King-Dejardin, Former senior staff of ILO (Geneva) and author of the 2018 ILO report, “The Social Construction of Migrant Care Work.”
[1] King-Dejardin, A., 2019, The social construction of migrant care work, Geneva: ILO https://www.ilo.org/global/topics/labour-migration/publications/WCMS_674622/lang–en/index.htm
*Learn more about the ILO Bureau of Gender Equality here
- Published in COVID 19, Migrant Care Workers
“Being at Home” is Not Free – Making Informal Care Provision Visible and Providing Support During the Pandemic

The Japanese Government responded to the COVID 19 crisis by declaring a state of emergency and announcing an economic stimulus of 108 trillion yen, 6 trillion of which is allocated to households and small to midsized businesses. However, care work is not mentioned in this state of emergency. In the face of this pandemic, the government should be taking into account the increased burden of home care that is brought on in addition to the concerns regarding the collapse of medical care.
Although medical care is very important, home goes beyond medical care in terms of responsibilities. Take, for instance, an elderly person that has home aid providing essential forms of care – preparing meals, etc. These care workers are taking on huge risks and burdens, and the fact that neither policymakers nor the press are paying attention to this is problematic.
Additionally, as hospitals are overrun with the sickest patients, many those that have contracted COVID-19 are forced to stay home, leaving relatives, especially women, to care for them without the proper PPE or the vigorous sanitation needed. This will result in further spread of the virus, and each household will take on a similar pattern to what has been seen on cruise ships. Furthermore, in Japan, many people live in small homes, making it impossible to create “quarantined zones” within the home. There is also the consideration that many of those in isolation do not have a member of the household to do the shopping. Those individuals are left without access to basic provisions and this is especially the case amongst those that live alone.
Although Prime Minister Abe has thanked the medical staff and truck drivers, he has failed to mention the family care members and the important role they play, which might indicate that family care is seen as a mere obligation, as plentiful as water or air.
The government in South Korea has taken on a much different approach, taking note of these needs, it responded by providing provisions to those that are isolated at home and are unable to go shopping. These provisions show that publicly fulfilling care needs may help in preventing the spread of the disease.
Japan technically has similar measure in place under the Japanese Infectious Disease Control Law, which requires that the government must provide necessities in order to enable individuals to stay home to prevent the spread of infection. However, in actuality, this has not been the case. In Osaka, a modern welfare policy exists to provide coupons for residents for food delivery from local restaurants, helping both those in isolation and local small businesses. This is an example that could be replicated on a national scale with the cooperation of the government and private sector.
I created a survey with colleague Mr. Nanami Suziki to investigate the ease in which people can self-isolate. The survey was distributed through the internet in April 8th and as of April 12th , 330 responses were recorded. These results indicate that domestic work within the home is on the rise, with increasing burdens for those responsible for these tasks within the home. Furthermore, the increased domestic workload is putting strain on those who are remotely working from home.
Survey results show that although in many cases both men and women work remotely, women more often end up taking on all additional home responsibilities imposed by the pandemic, including homeschooling for the children.
As a result, many women are taking leave from their jobs, are working longer hours, and are becoming sleep deprived. Additionally, the increased family stress can lead to domestic violence. Policymakers and the press need to be more attentive to these increased burdens.
Steps can be taken to alleviate this situation, beginning with making care work visible and providing compensation. Further, ensuring employment and income those providing care for individuals in quarantine. This would follow the example set by South Korea in which those that cannot be paid to take leave can apply for living expenses to be supported through the government. As it stands now, Japanese relief policies fail to recognize the increased care burden being faced in the home, primarily by women.
Further, the government should respond by distributing lunch boxes to children that are not able to attend school due to closures, helping those children living in poor households that rely on school lunch. It is also important to support to the continuation of programs that are providing this sort of social care.
There have been some positive results from this situation, such as more family time and communication. Economy is only one aspect of life and moving forward, care work should be made visible in order to create a shift in society that mainstreams the value of “life” over “economy.”
* Thanks to Asahi Okamoto, Kaori Yamamoto, and Yoon Sodam.
This blog is authored by Emiko Ochiai who is a Professor of Sociology at Kyoto University.
Originally published in Japanese to the Women’s Action Network on Monday, April 13, 2020
- Published in COVID 19, Japan, Policy, South Korea
Those unprotected by the “economic stability shield”

This brief note raises two issues: First, the widening of gender inequalities in unpaid care work and second, the potential gendered outcomes of rising formal and informal unemployment in the affected sectors in Turkey.
Market production is at a halt, yet women are working overtime
What sustains human life, as we all know, cannot be maintained solely by market purchased goods and services. Our lives are constantly reproduced within households. The overwhelming majority of women are involved in the provisioning of the most indispensable items needed to sustain our lives and enhance their quality.
We are told that economies are experiencing a “sudden stop”. While some businesses temporarily close their doors, there is full capacity production ongoing at our homes. In technical terms, excess capacity in market production is rising, while women are working overtime. Some forms of housework now require more attention and diligence for hygienic purposes than ordinary times. Sterilizing market purchased goods, washing the clothes and cleaning the house more frequently are now necessary. The shutdown of nurseries, kindergartens and schools increased childcare work burden. Adult and elderly care burden also increased. Turkey has banned people aged 65 or older from leaving their homes on March 21 and people aged 20 or younger very recently. These developments significantly increase women’s workload. The family has already been central to the welfare regime of Turkey. Care of children, elderly and people with disabilities have been overly dependent on families. We observe once again, the family-centered welfare regime shifts the care burden onto the families.
The unemployed and informal workers
As of December 2019, prior to the pandemic, nearly 4.3 million people were unemployed. It is assumed that approximately 9-10 million people will be unemployed after the pandemic. The unemployed and their household members–nearly half the population in Turkey—are at serious poverty risk.
“Economic Stability Shield” Package consists mostly of policies that aim to help the firm owners and ignores the most vulnerable segments: the long-term unemployed, first-time job seekers and the recently employed.
The other segment of the population overlooked by the Package is the unregistered or informal workers. More than five million workers, are working informally, and hence without social security, in Turkey.
It is clear that small and medium-sized companies, where informal work is widespread will be more adversely affected by the crisis. Accommodation and food (tourism sector at large), retail trade, and textiles and apparel will be most affected due to the pandemic. We estimate that 650 thousand informal workers in these three sectors are in danger of losing their jobs. In addition, over 700 thousand informal workers from the remaining sectors are estimated to lose their jobs.
The three sectors that are most affected by job losses make up almost a quarter of non-agricultural women’s employment. Even if we assume that there would be no employer discrimination and employers act in accordance with these current rates during layoffs, around 700 thousand women will lose their jobs, and around 190 thousand of those will not have any access to social security benefits since they have been working informally.
Our lives are upside down now and the future does not look bright at all. However, it is not the time to be pessimistic either. As we all know, all inequalities are socially constructed; their elimination will be too. If our struggle to rearrange our lives during and after this epidemic; will be towards more solidarity and towards an egalitarian society, we can start by deciphering all kinds of inequality, discrimination and exploitation inside and outside our homes.
This blog was authored by Emel Memiş, Department of Economics, Ankara University, KEFA and IAFFE member; Murat Koyuncu, Department of Economics, Boğaziçi University and Şemsa Özar, Department of Economics, Boğaziçi University, KEFA member, member and former president of IAFFE
- Published in Gender Inequalities, Turkey, Unpaid Work
Domestic and Care Workers Under COVID-19
By definition, domestic workers are an essential part of the global care workforce. According to the ILO, there are 70 million domestic workers over the age of 15 working directly for private households. They therefore make up roughly 22.7% of the global care workforce (which number 308,6 million).[1] Since its foundation in 2013, the International Domestic Workers Federation (IDWF) has worked with global unions and key audiences with the aim of including home care workers into the global agenda on “care” and to fight for the improvement of their living and working conditions.
Work in the care sector changes rapidly due to aging populations in the west and the more industrialized part of Asia. Financial demands on families who rely on unpaid care work, or the reliance by governments on private and not-for-profit sectors to play an increasing role in providing services. In Asia, most governments deny labour rights and working conditions, particularly for migrant workers, In the west, there is an increasing number of undocumented migrant domestic workers and they do not enjoy labour rights protection due to their vulnerable status. In recognition of the challenges in care work, in 2018 the IDWF Congress adopted two Resolutions (No. 3 & 4) to guide the Federation’s work and address global demands on developing inclusive care systems, special protection programs, and special attention to undocumented and migrant worker’s needs.
The new coronavirus pandemic has impacted all regions for more than three months. Domestic, household and care workers are on the frontlines in keeping families and communities healthy, but they are also most at risk. COVID19 has increased the vulnerability of the sector, which is already and broadly characterized by lack of protections, social security or recognition in many places of the world.
The IDWF consists of 74 affiliates in 57 countries, representing almost 600,000 domestic workers. Since the pandemic began, the IDWF has been actively engaging with affiliates in all regions to monitor the situation on the ground. In many countries, workers are experiencing a substantial increase in workload to ensure cleanliness and hygiene; or in taking care of older people and people with existing medical conditions.
The most critical issues identified:
– Domestic and care workers, especially the live-out/ part time are the most vulnerable group. They cannot move around and lose their jobs due to the lockdowns and social distancing rules, or their employers no longer call them in to work. Many have endured this situation for several weeks while others are losing their jobs with no prospects of finding new sources of income.
-Without income, migrant workers are especially vulnerable as they try to survive in the destination countries. In many countries, migrant workers are not eligible for medical services and hence do not get COVID-19 tests, places for quarantine or medical treatment when needed.
-Workers from rural areas working in the cities, cannot return to their families, or access relief packages provided by local governments.
-The lack of medical and social protections benefits renders domestic and care workers unprotected even when they are sick or need to be quarantined with no remuneration. IDWF and Affiliates are monitoring the mortality rates of members, a difficult task as many governments do not test or report incidents.
-Despite the essential work, domestic and care workers face increasing discrimination during the pandemic. Many workers report for being blamed for bringing the virus into their employers’ homes.
-The ability of domestic workers unions to keep their offices functioning is also compromised during quarantine or semi-quarantine time. Many unions are able to pay for the basic services and provide essential support (i.e. information, food baskets, training) from income previously generated. It is essential that union offices keep operating and maintaining their services for a range of situations that go from unfair dismissals to gender based violence.
In this situation, most organizations have shifted or stopped normal activities. With exception to those in North America and Europe, most organizations are struggling to find ways and means to address emergencies. Some countries have included domestic workers in their relief programs while others have joined hands with allies to demand governments to give out wages /cash, food, masks, sanitizers, places for quarantine. As the pandemic continues, so will the crisis on the ground.
Based on its assessment, the IDWF will continue to do research and collect data to inform advocacy. The IDWF will also set up a solidarity fund to address some of the most critical needs to enable domestic/care workers –and their families– to cope and survive with COVID-19.
[1] ILO (2018), Geneva. Care Work and Care Jobs For the Future of Decent Work.
Contributed by Sofia Trevino, Sustainability Advisor for International Domestic Workers Federation (IDWF) and the Project Manager for Women in Informal Employment Globalizing and Organizing (WIEGO)
Relevant Links:
IDWF: Decent work for Domestic Workers: Eight Good Practices from Asia
In IDWF site, resources on care work (books, articles, websites, audio)
An essay collection on Care economy: Three Years of Collective and Global Learning About Care
ILO Decent Work in the Care Economy
Care Needs and Migration for Domestic Work: Poland and Ukraine
Migrant Domestic Workers: Promoting Occupational Safety and Health
Expanding Social Security to Migrant Domestic Workers
IDWF Resolutions adopted by the 2nd Congress in 2018, Cape Town, South Africa
ILO: Social Protection for Domestic Workers: Key Policy Trends and Statistics
ILO World of Work Magazine: Violence at Work
Decent Work for Domestic Workers: Eight Good Practices from Asia, ILO and IDWF
Why We Care about Care: An Online Moderated Course on Care Economy, UN Women
Research Network of Domestic Workers Rights
WIEGO:
UN High Level Panel Report on Child Care by Rachel Moussié, Deputy Director of WIEGO Social Protection Programme.
Counting the World’s Informal Workers: A Global Snapshot
The ILO – WIEGO policy brief series on childcare for informal workers
Sofia Trevino is the Sustainability Advisor for International Domestic Workers Federation (IDWF) and the Project Manager for Women in Informal Employment Globalizing and Organizing (WIEGO)
- Published in Child Care, COVID 19, Domestic Workers, Policy Briefs & Reports