A Gender Lens on COVID-19: Investing in Nurses and Other Frontline Health Workers to Improve Health Systems

In a recent CGD blog post, author Megan O’Donnell highlighted seven areas where long-run, gender-responsive thinking can help to insulate against the consequences of pandemics like COVID-19 and their disproportionate impacts on women and girls. Here we take a deeper dive into one of those areas: the promotion of a gender-equal global health workforce in which the occupations where women predominate, such as nursing and community health work, are valued, prioritized, and properly resourced.
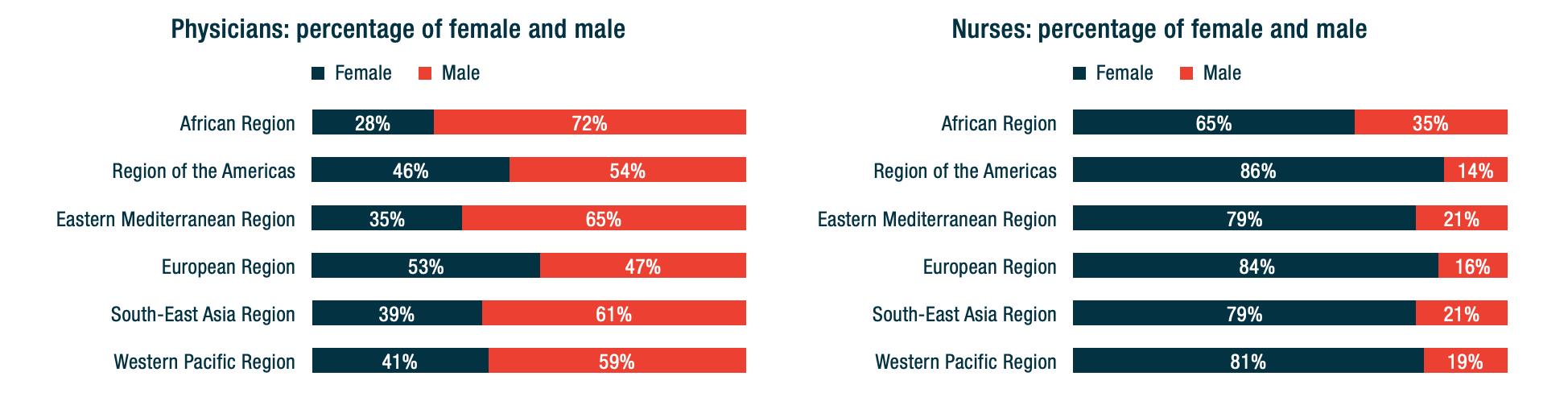
Worldwide, women make up anywhere from 65 percent (Africa) to 86 percent (Americas) of the nursing workforce. Their jobs are critical to the health, safety, and security of communities on any given day, and particularly in times of a global pandemic. And yet, more obviously now than ever before, we face a global nursing shortage. To address this critical short fall and ensure sufficient numbers and distribution of health workers to provide both emergency and routine care in time of crisis, governments need to increase and improve their long-term investment in nurses, including by addressing gender gaps in the health workforce.
- Published in COVID 19, Gender Inequalities, Healthcare
How Will COVID-19 Affect Women and Girls in Low- and Middle-Income Countries?

Policymakers should be thinking—and worried—about how COVID-19 is expected to disproportionately affect women and girls. Gender inequality can come into even starker focus in the context of health emergencies. With COVID-19 continuing to spread, what do we see so far—and what can we expect in the future—in terms of the impacts on women and girls?
Wenham, Smith, and Morgan discuss gendered impacts in their article, “COVID-19: the gendered impacts of the outbreak,” in the Lancet. Women appear to be less likely to die from COVID-19: “Emerging evidence suggests that more men than women are dying, potentially due to sex-based immunological or gendered differences, such as patterns and prevalence of smoking.” But keep in mind that “current sex-disaggregated data are incomplete, cautioning against early assumptions.” In other research, data from 1,000+ patients in China show that “41.9% of the patients were female.” (Guan and others 2020). But beyond these direct effects, most of the other impacts affect women negatively and disproportionately.
Wenham, Smith, and Morgan highlight that women will be more affected in places with more female health workers. In an analysis of 104 countries, Boniol and others (2019) show that women form 67 percent of the health workforce (see the figure below). In China, “an estimated 3000 health care workers have been infected and at least 22 have died” (Adams and Walls 2020). As the pandemic spreads, the toll on women health workers will likely be significant.
Figure. Gender distribution of health workers across 104 countries
Source: Boniol and others (2019)
Here are other areas highlighted by Wenham, Smith, and Morgan:
– School closures are likely to have a differential impact on women, who in many societies take principal responsibility for children. Women’s participation in work outside the home is likely to fall. (My colleagues Minardi, Hares, and Crawfurd have written about other impacts of school closures during an epidemic.)
-Travel restrictions will affect female foreign domestic workers. Of course, they also affect male migrants. The distribution will vary by country. Research by Korkoya and Wreh (2015) found that 70 percent of small-scale traders in Liberia are women, so domestic travel restrictions during the Ebola outbreak disproportionately affected women.
-Health resources normally dedicated to reproductive health go towards emergency response. During the Ebola outbreak in Sierra Leone, for example, the “decrease in utilization of life-saving health services translates to 3600 additional maternal, neonatal and stillbirth deaths in the year 2014-15 under the most conservative scenario” (Sochas, Channon, and Nam 2017). In my own research (with Goldstein and Popova), we found that the disproportionate loss of health workers in areas that had few to begin with would likely lead to higher maternal mortality for years to come.
-When women have less decision-making power than men, either in households or in government, then women’s needs during an epidemic are less likely to be met.
Here are four additional concerns:
-Sexual health: During the school closures of Sierra Leone’s Ebola outbreak, “a reported increase in adolescent pregnancies during the outbreak has been attributed largely to the closure of schools.” (UNDP 2015). Bandiera and others find that in villages highly disrupted by Ebola, girls were “10.7 percentage points more likely to be become pregnant, with most of these pregnancies occurring out of wedlock.” A United Nations report gives an even higher estimate of 65 percent. The absorption of health resources by emergency response may also lead to disruptions in access to reproductive health services.
Many girls didn’t return to schools once they reopened, and there were increases in unwanted sex and transactional sex. (Notably, Bandiera and others also find that girls in villages where there were established “girls’ clubs”—safe spaces for teenage and young adult girls to gather and get job and life skills—before the epidemic experienced fewer of these adverse effects.)
-Intimate partner violence rises in the wake of emergencies: Parkinson and Clare document a 53 percent rise in the wake of an earthquake in New Zealand and nearly a doubling in the wake of Hurricane Katrina in the United States. Mobarak and Ramos find that in Bangladesh, increased seasonal migration reduces intimate partner violence, at least in part because women spend less time with the potential perpetrators of that violence. Travel restrictions may be expected to have the opposite effect.
-The burden of care usually falls on women—not just for children in the face of school closures, but also for extended family members. As family members fall ill, women are more likely to provide care for them (as documented during an Ebola outbreak in Liberia, with AIDS patients in Uganda, and in many other places), putting themselves at higher risk of exposure as well as sacrificing their time. Women are also more likely to be burdened with household tasks, which increase with more people staying at home during a quarantine.
-As Mead Over and I have discussed, health crises can trigger economic crises. Economic crises affect women disproportionately, particularly in low-income countries. Sabarwal and others found that men’s labor force participation remained largely unchanged during economic crises, whereas women’s labor force participation rose in the poorest households and fell in richer households.
-Last week, the World Health Organization declared that “this is the first pandemic caused by a coronavirus.” There have been more than 168,000 confirmed cases and more than 6,600 deaths in 148 countries as of publication of this blog. The impact of this pandemic will be felt for years to come. As women are often disproportionately affected by the follow-on effects of the disease, we have to make sure that we keep women’s rights and needs front and center in our responses. A first step in doing that is making sure that women are a central part of the teams designing those responses.
Contributed by David Evans, senior fellow at the Center for Global Development, working on education, health, and social safety nets.
This post benefitted from comments provided by Susannah Hares, Megan O’Donnell, Emily Christensen Rand, and Rachel Silverman.
Original blog published on Center for Global Development website March 16, 2020, see here for the original posting
Reposted with permission from David Evans, senior fellow at the Center for Global Development
- Published in COVID 19, Healthcare